
While we wait for further results from phase 3 trials, it’s clear that supply of any potential COVID vaccine would initially be limited.
Local authorities will need to prioritize distribution to specific groups, at least at first. So how might they make these decisions?
The general consensus is people with very high risk of exposure to COVID, such as workers in front line health-care and quarantine facilities, should be first.
Less clear is the question of who should be next. This group could include people with work, demographic or health characteristics that put them at high risk of either exposure or serious disease.
Following a National Cabinet meeting on Friday, the federal government indicated the elderly and vulnerable would be a priority group.
Here’s why prioritizing older people to receive the earliest COVID vaccines is a good idea.
First, a bit of background
Vaccines work in several different ways, providing benefits to the individual and the community.
An obvious individual benefit is that vaccines can prevent infection in the person who is vaccinated. But vaccines can also reduce the amount of virus a person makes if they do end up becoming infected. This can reduce severe disease and reduce their likelihood of transmitting the virus to others.
All this leads to benefits for the community. If vaccine uptake is high enough and transmission is reduced, our collective (or herd) immunity can be used like a fire break. It blocks pathways of virus transmission and protects vulnerable people from infection, even when those people are not vaccinated.
Severe disease due to COVID is a critical health issue, with the potential to put significant stress on health-care systems and resources. But if vaccine supply is limited, do we:
- directly reduce severe disease by giving the vaccine to those most at risk, such as older people
- indirectly reduce severe disease by vaccinating the people most likely to get sick and transmit the virus, such as certain groups of younger people
- use a mix of both strategies?
The question is, how can a limited supply of vaccine have the most impact?
Vaccines and the elderly
As we get older, our immune cells can become more difficult to activate, in response to the natural aging process or other factors like chronic inflammation. As a result, vaccines often don’t protect older people as well as younger people.
Importantly, a phase 1 study with a BioNTech/Pfizer COVID vaccine candidate showed the size of the immune response was lower in older people, which may suggest reduced protection.
Because of this, the public might think prioritizing vaccines for older people is a bad idea. Why give a vaccine to people who it won’t work as well in? But we should explore older people as a priority group for several reasons.
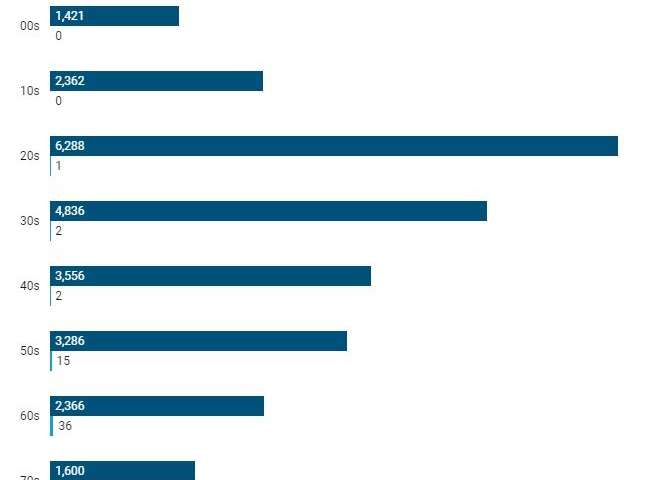
First, older people are bearing the brunt of severe disease from COVID. In Australia, nearly half of severe cases requiring intensive care, and more than 90% of deaths, have been people over 65.
Second, a potential vaccine may not protect as well in older people, but it should protect to a degree. As an example, the flu vaccine provides 60-70% protection in the general community, dropping to 30-40% protection in people over 65—but even at that rate it’s still protecting a substantial number of older people.
Third, where a potential vaccine doesn’t prevent infection, it could still reduce severe disease. For example, in one study, the flu vaccine reduced the rate of severe disease in vaccinated people by 23% regardless of age group.
A modest improvement in cases or severe disease in older people could have a big impact on the overall burden of disease and death.
In particular, aged-care facilities should be considered a top priority. This environment is high risk, combining people at very high risk of severe disease and high-density accommodation. Vaccinating aged-care staff could prevent the virus getting in and vaccinating residents could minimize the consequences if it did.
Finally, some vaccines may work well in older people. For example, the Shingrix vaccine stunned the research community in 2015 by demonstrating over 90% protection against shingles in older people—a vast improvement on the previous Zostavax vaccine which provided only 50% protection.
While initial supply will be limited, we may end up with access to multiple COVID vaccines, which could allow us to prioritize potent vaccines for older people.
Big decisions take a village
In any scenario, tackling complex questions around vaccine distribution will require specialist knowledge from across many disciplines.
We need to understand how the virus spreads in a given population, how the vaccine works in different groups within that population, who might be hesitant about the vaccine, how we can deliver the vaccine to a wide variety of people and many other factors.
Importantly, we’re still learning about this virus. It behaves differently in different communities, due to different environments, demographics, biology and behaviors. Strategies may differ in different regions and must adapt with our evolving understanding of the virus. There won’t be a “one size fits all” approach.
It’s also vital to keep in mind that a vaccine won’t be a silver bullet. Vaccines are not 100% protective and will take time to roll out. Public health measures such as rigorous testing, hand-washing, mask-wearing and a level of social distancing will remain important for some time.
Source: Read Full Article